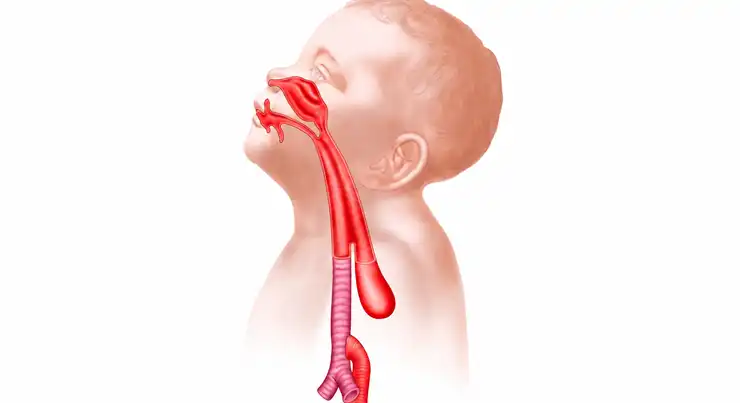
Tracheoesophageal Fistula (TEF) in children is a congenital condition in which there is an abnormal connection between the trachea (windpipe) and the esophagus (food pipe). In many cases, it occurs along with esophageal atresia, where the esophagus does not develop into a continuous tube.
Because of this abnormal connection, food, milk, or saliva can enter the airway instead of the stomach, leading to choking, breathing difficulties, and repeated lung infections. TEF is usually detected soon after birth and requires prompt medical attention.
With early diagnosis and specialized pediatric surgery, most babies with TEF can recover well and lead healthy lives.
The symptoms of TEF usually appear shortly after birth, especially during feeding.
Common symptoms of Tracheoesophageal Fistula in children include:
If left untreated, aspiration of milk into the lungs can lead to serious complications.
TEF develops during early fetal growth when the trachea and esophagus fail to separate properly.
Possible causes and contributing factors include:
In most cases, the exact cause is unknown and is not related to anything parents did during pregnancy.
There are several types of TEF depending on how the trachea and esophagus are connected.
1. Esophageal Atresia with Distal Tracheoesophageal Fistula: This is the most common type. The upper esophagus ends in a blind pouch, while the lower part is connected to the trachea.
2. Pure Esophageal Atresia: The esophagus ends blindly without any connection to the trachea.
3. H-Type Tracheoesophageal Fistula: The trachea and esophagus are connected by a small passage, but the esophagus remains continuous. This type may present later in infancy or childhood.
4. Proximal Tracheoesophageal Fistula: The upper part of the esophagus is abnormally connected to the trachea.
5. Double Tracheoesophageal Fistula: A rare form in which both the upper and lower esophagus communicate with the trachea.
Certain factors may increase the likelihood of TEF.
Risk factors include:
Many babies with TEF also have other congenital conditions that require evaluation.
Without timely treatment, TEF can lead to several serious complications.
Doctors diagnose TEF using clinical evaluation and imaging studies.
Diagnosis may include:
Many cases are suspected before birth due to excess amniotic fluid or absent stomach bubble on prenatal ultrasound.
TEF requires surgical correction, usually soon after birth.
Before surgery, the baby may need:
The surgeon closes the abnormal connection between the trachea and esophagus and reconnects the esophageal segments if needed.
The goals of surgery are to:
In selected cases, thoracoscopic (keyhole) surgery may be an option depending on the baby’s condition and anatomy.
Recovery varies depending on the severity of the condition and associated abnormalities.
Parents are usually advised to:
Some babies may require temporary tube feeding during recovery.
Helpful care measures include:
Long-term follow-up is important for detecting reflux, swallowing difficulties, or esophageal narrowing.
Seek medical attention immediately if your child develops:
Early evaluation can prevent serious complications and improve outcomes.
Yes, TEF is a congenital condition that develops during fetal growth.
Yes, most babies require surgery, and many recover well with timely treatment and follow-up.
If left untreated, it can lead to serious breathing problems and lung infections, making early treatment essential.
Most children gradually learn to feed normally, although some may need temporary feeding support or treatment for swallowing difficulties.
Yes, follow-up is important to monitor feeding, growth, reflux, and esophageal function.
Yes, some children with TEF may also have heart, kidney, spinal, or gastrointestinal abnormalities.
Dr. Muni Varma is an experienced Pediatric Surgeon & Neonatal Surgeon with expertise in treating Tracheoesophageal Fistula (TEF) and other complex neonatal surgical conditions. Using advanced diagnostic techniques and modern surgical approaches, he provides comprehensive care from newborn stabilization to definitive repair and long-term follow-up. His focus on safe surgery, individualized treatment, and multidisciplinary care helps improve feeding, breathing, and overall development while minimizing complications. With timely intervention and expert management, children with TEF can achieve excellent outcomes and a better quality of life.
